Research
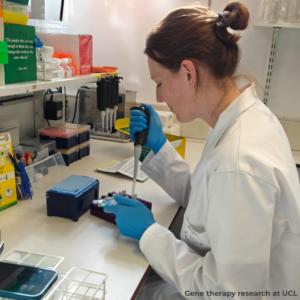
At Cavernoma Alliance UK, our vision is to find a cure for cavernoma. To achieve this, we promote research to develop new treatments and advocate for UK access to emerging therapies. Our primary role is to bring people together to develop research proposals and support them through patient and public involvement (PPI) to secure funding, such as from the NIHR. We have also directly funded research, including a novel gene therapy project at UCL.
UK research
CAUK’s vision is to find a cure for cavernoma. To help make this a reality, we’re working with three leading UK universities to do this.
Using existing drugs to treat cavernoma
At the University of Edinburgh we are working closely with Professor Rustam Al Shahi Salman on a proposal building on the CARE study. It will explore whether aspirin could be safely repurposed to treat people with cavernoma and is awaiting a funding decision.
Developing a gene therapy for familial cavernoma
At the UCL Institute for Women’s Health we are working with Professor Rajvinder Karda and Dr Ellie Chilcott on an early stage gene therapy project that aims to address the genetic cause of cavernoma. This work is co funded by CAUK, Cavernoma Ireland and a philanthropist.
Uncovering new genetic causes
At the University of Liverpool we are supporting Professor Ben Goult who is studying why some people inherit cavernoma even when they test negative for known CCM genes. Working with The Walton Centre, the team has identified a candidate protein, TLNRD1, that may help explain how some cavernomas form.
If you are a researcher working on cavernoma, we would welcome a discussion about patient and public involvement (PPI). Contact us at admin@cavernoma.org.uk.
Overseas research
There is a great deal of progress being made internationally, especially in the United States. Our sister organisation in the US, Alliance to Cure, shares up to date information on global research, treatment pipelines and laboratory work. Explore:
Historical UK research
Cavernomas: A Randomised Effectiveness (CARE) Study
Results were published in April 2024 in The Lancet Neurology. Led by our Advisory Board Chair Professor Rustam Al Shahi Salman with CAUK support, this pilot showed that a full randomised trial comparing surgery plus medical care with medical care alone is feasible. Thirty hospitals gained approvals and twenty eight took part. Seventy two participants were recruited and followed up. During the study, two of the 33 people who had surgery and medical care experienced a stroke, and two of the 34 who had medical care alone experienced a stroke. The pilot identified what helped and hindered recruitment, paving the way for a larger international trial. More information: www.ed.ac.uk/care-study
James Lind Priority Setting Partnership
From 2014 to 2016 CAUK convened patients, carers and clinicians to agree the top unanswered questions about cavernoma in the brain and spine. The top ten priorities include whether treatment improves outcomes, how cavernomas begin and develop, risks of bleeding, the role of medicines, triggers for bleeding or seizures, and the value of monitoring. The Cavernoma Priority Setting Partnership has guided research in the UK and internationally.
Guidelines for treatment
In 2012 UK experts produced guidance that remains a useful reference for clinicians and people affected by cavernoma.
Read the document.
With thanks
Our thanks go to Professor David White, CAUK’s former Scientific Advisor and long-standing Chair of Trustees, whose contributions made much of CAUK’s historical research possible. David retired in 2023, and we remain deeply grateful for his leadership and commitment to advancing cavernoma research.
Information for researchers
Prevalence
Asymptomatic brain cavernoma is estimated between 1 in 625 and 1 in 217 in the UK. Symptomatic cavernoma is about 1 in 2,703. Around five percent of cavernomas are found in the spine. Approximately twenty percent are familial with a genetic cause.
Natural history references
Key overviews include Al-Shahi Salman et al. Lancet Regional Health 2025, Taslimi et al. Neurology 2016 and Horne et al. Lancet Neurology 2016, alongside a paediatric familial data paper in Neuroradiology 2023.
Clinical endpoints and biomarkers
Typical endpoints include symptomatic intracerebral haemorrhage and focal neurological deficits, with secondary outcomes such as quality of life, mood, seizures and MRI based measures including SWI, QSM, DCEP, lesion characteristics and de novo lesions. Biomarker work is ongoing across blood, imaging, stool and urine. See Alliance to Cure’s biomarker pages.
Models and tools
Available models include global knockout, genetically sensitised and Cre lox inducible mouse models. Relevant cell lines include induced pluripotent stem cell models of CCM.
Biorepositories
Alliance to Cure maintains a cavernoma DNA and tissue bank.
Existing treatments
Direct interventions remain microsurgical excision or stereotactic radiosurgery where appropriate. Non surgical treatments and novel agents are in development internationally.
See treatments in development.
Work with us
CAUK regularly partners as a PPI lead or collaborator, convenes patient advisory groups and supports recruitment materials and community engagement. If you are planning a study please contact us at admin@cavernoma.org.uk.